Q&A with NBER research associates Ellen Meara and Richard Frank
The NBER is pleased to feature a Q&A with research associates
Ellen Meara and
Richard Frank, both of Harvard University, whose research on differing aspects of disability are summarized earlier in this issue.

Q (Meara & Frank): Each of your papers in this issue touch on the links between health, occupation-specific factors, and SSDI application rates. How do you see the evolving health and/or employment dynamics in the US affecting trends in SSDI application rates?
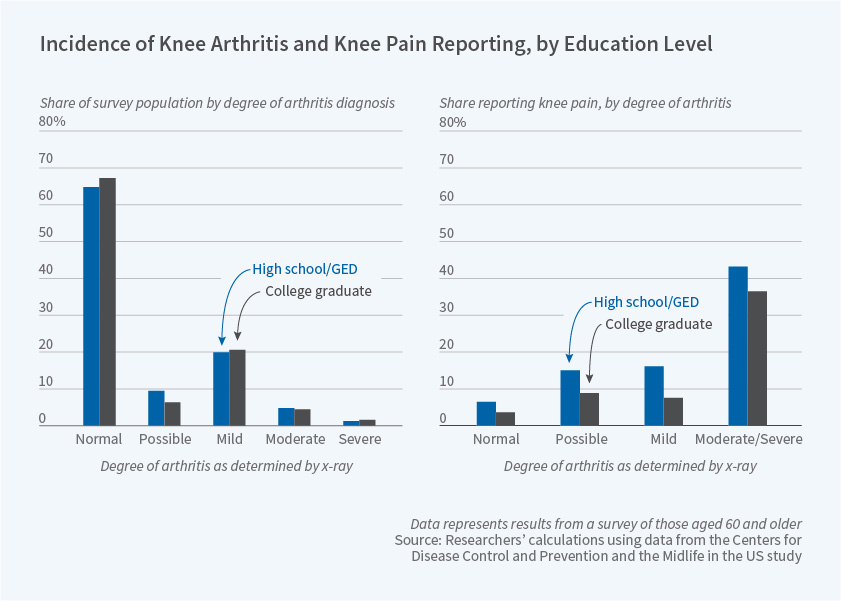
A (Meara): In our paper, we saw that two workers with identical health on objective measures like an x-ray or MRI of the knee can report very different levels of pain in ways that are linked to education. These educational differences tracked differences in physical demands of occupations more likely among high school graduates than college attendees. Although automation lessens the physical demands of some occupations, the fastest growing occupations in the US, home health care and other personal care jobs, are both physically demanding and hard to automate. As more workers move into physically demanding service sector jobs, we can expect musculoskeletal conditions to remain an important source of disability and claims for years to come.
A (Frank): In our research, we focus on the impacts of mental illnesses on labor force participation, occupational choice and SSDI application rates. We show that people with mental illnesses have lower rates of labor force participation. When they do work they are concentrated in jobs that involve routine cognitive and interpersonal skills. They also cluster in low wage occupations. These are the jobs that have been disappearing as a result of technical change and are projected to continue to be subject to automation. The result is that SSDI application rates for people with mental illnesses have grown faster than those for the working age population generally. These results suggest that people with mental illnesses will be at higher risk of loss of employment opportunities than otherwise similar people.
Q (Meara): Your current work explores chronic pain. Prescription opioids can be used to treat chronic pain, but they carry a risk of abuse, which can lead to other health problems. From your past work, what do we know about how the rise of prescription opioids has affected SSDI enrollment?
A: In light of the crisis of opioid overdose deaths, the risks of prescription opioids are now well known and opioid prescribing is declining. Some worry that curtailing opioid prescriptions could leave some workers with unmanageable pain, in turn increasing rates of disability application. To get at this question, we compared disability application rates in states with steadily rising prescription opioid receipt between 2001 and 2015 to states like Florida, where prescription opioid receipt peaked in 2010 and fell rapidly afterwards. Within an area, periods of high prescribing were unrelated, or in some analyses, positively related to disability application rates. This is good news for disability programs in the sense that we do not expect disability applications to rise, and indeed they may fall, as opioid prescribing becomes less common.
Q (Frank): While your current work focuses on mental health and SSDI receipt, many people with severe mental illness are also eligible for Medicare, Medicaid, or both. What does your previous work tell us about the provision of health care for this vulnerable group?
A: Medicaid has always been an important source of health care coverage for people with severe mental illnesses. The Affordable Care Act's Medicaid expansion disproportionately offered coverage for people with mental illnesses that were almost twice as likely to be uninsured as those without those conditions. Because severe mental illnesses develop early in life many people with severe mental illnesses were single childless adults. That meant that prior to the ACA they were typically ineligible for Medicaid coverage. For this reason there has been an expansion in the ability to get care for these people.
Q (Meara & Frank): Which related areas of research appear most promising or most critical for future study?
A (Meara): While the broad contours of opioid-related risks around overdose and addiction are well documented, the health and disability consequences of prescription and illicit opioids remain unclear. For example, US mortality rates rose and life expectancy at birth fell between 2014 and 2017 in part, due to overdose deaths, but deaths rose for causes like cardiovascular disease and alcohol related cirrhosis as well. Such trends suggest the underlying prevalence of health problems and disability in the US has been rising. An appropriate response to such trends depends on the exact causes of health deterioration. The remedy for deaths resulting directly from opioid use (e.g. increasing access to products like naloxone that reverse the lethal effects overdose) differs from an effective response to deaths that occur indirectly due to opioids (e.g. improving self-management of chronic physical conditions). But rising morbidity and mortality may have little to do with opioids, and an entirely different solution may be required if rising morbidity and mortality are a symptom of a general decline in health and well-being as technology advances reduce opportunities, and optimism, for less educated workers. Research should seek to better understand trends in morbidity and mortality, and the ways in which some subgroups and communities in the US are hit harder than others.
A (Frank): There have been many efforts aimed at developing policies and interventions aimed at reducing the number of people on SSDI by helping them return to the labor force. Those have not been successful. Far more promising are recent clinical developments aimed at intervening early in the course of a severe mental illness to keep people engaged in work and schooling. A promising avenue for economic and policy research is developing the payment systems and financing arrangements that will support implementation of those interventions.